Flupentixol decanoate 20 mg/ml.
Excipients/Inactive Ingredients: Thin vegetable oil.
Pharmacotherapeutic classification: Antipsychotics, thioxanthene derivatives. ATC-code: N 05 AF 01.
Pharmacology: Pharmacodynamics: Flupentixol belongs to the thioxanthene group of antipsychotics.
The antipsychotic effect of these drugs is related to their dopamine receptor blocking action, but blocking of the 5-HT-receptor may also contribute.
In vitro and in vivo, flupentixol has a high affinity for both dopamine D1 and D2 receptors, while fluphenazine in vivo is almost selective for D2. Like flupentixol, clozapine has a similar affinity for D1 and D2 receptors both in vitro and in vivo. Flupentixol has a high affinity for α1-adrenoreceptors and 5-HT2 receptors, although less so than chlorprothixene, high-dosage phenothiazines and clozapine, while having no affinity for cholinergic muscarinic receptors. It has weak antihistaminergic properties only and no α2-adrenoreceptor-blocking action.
Flupentixol is a potent antipsychotic in all behavioural models for antipsychotic (dopamine receptor-blocking) activity. There is correlation between in vivo test models, the affinity for D2 binding sites in vitro and the mean daily oral dose of the antipsychotic.
Perioral movements in rats depend on D1 receptor stimulation or blockade of the D2 receptor population. Onset of these movements can be prevented by flupentixol. In addition, the results of trials in monkeys show that oral hyperkinesias are more related to D1 receptor stimulation and less to D2 receptor supersensitivity. This leads to the assumption that D1 activation lies behind similar activities in humans, i.e., dyskinesia. Accordingly, D1 blockade is considered beneficial.
Like most other antipsychotics, flupentixol increases the serum levels of prolactin in a dose-dependent manner.
Pharmacological studies have shown that flupentixol decanoate suspended in oil has prolonged antipsychotic activities, and that the amount of substance required to maintain a specific effect long-term is considerably lower with the solution for injection than with daily ingestion of oral doses. Only very high doses of flupentixol decanoate can briefly prolong the sleeping time induced by alcohol and barbiturates in mice, which indicates a very weak sedative action in clinical use.
In clinical use, Fluanxol Depot is designed for maintenance treatment of patients with chronic psychoses. The antipsychotic effect increases with increasing doses. In low to moderate doses (up to 100 mg every two weeks), flupentixol decanoate is not sedating, whereas some non-specific sedation may be expected following administration of higher doses.
Fluanxol Depot is particularly suitable in the treatment of apathetic, lethargic, depressed or poorly motivated patients.
With Fluanxol Depot, a continuous antipsychotic therapy is ensured, which reduces the rate of recurrence because of non-compliance of orally treated patients.
Pharmacokinetics: Absorption: Intramuscular injections produce peak plasma concentration (Tmax) within 3 to 7 days. At an estimated half-life of ca. 3 weeks (reflecting the modified release), steady state concentrations are achieved within approximately 3 months of repeated dosing.
Distribution: The apparent volume of distribution (Vd)β is approximately 14.1 L/kg. Plasma protein binding is approximately 99 %. Flupentixol passes the placental barrier.
Biotransformation: Flupentixol is mainly metabolised by sulfoxidation, side-chain N-dealkylation and conjugation with glucuronic acid. The metabolites show no antipsychotic activity. Concentrations of flupentixol found in the brain and other tissues are higher than those of its metabolites.
Elimination: The plasma elimination half life (t½β) is approximately 35 hours; systemic plasma clearance (Cls) is approximately 0.29 L/min. Cis(Z)-flupentixol is mainly excreted with the faeces, but also to some extent with the urine.
Small amounts of flupentixol are excreted into breast milk.
The average milk/plasma concentration ratio is 1.3.
Linearity: Pharmacokinetics are linear. After a dose of 40 mg flupentixol decanoate every 2 weeks, the Cmin of flupentixol is approximately 6 nmol/l at a steady state.
Elderly patients: Not investigated. For the very similar zuclopenthixol, however, the pharmacokinetic parameters are largely independent of the patient's age.
Renal impairment: Not investigated. Based on the previously mentioned elimination data, however, it is a reasonable assumption that renal impairment would not affect serum levels of flupentixol to any major degree.
Hepatic impairment: Not investigated.
Toxicology: Preclinical safety data: Acute toxicity: Flupentixol has low acute toxicity.
Chronic toxicity: Chronic toxicity studies have revealed nothing of relevance to the therapeutic use of flupentixol.
Reproductive toxicity: In fertility studies in rats, flupentixol slightly affected the pregnancy rate of female rats. Effects were seen at doses well in excess of those applied during clinical use.
Animal reproduction studies in mice, rats and rabbits have not shown evidence of teratogenic effects. Embryotoxic effects in terms of increased post implantation loss/increased absorption rates or occasional abortions were seen in rats and rabbits at doses associated with maternal toxicity.
Schizophrenia and allied psychoses, especially with symptoms such as hallucinations, paranoid delusions and thought disturbances along with apathy, anergy and withdrawal.
Posology: Adults: The individual dosage and the interval between injections should be tailored to the patient's condition.
Fluanxol Depot 20mg/ml: In the maintenance treatment the dosage range would normally be 20-40 mg (1-2 ml) every 2-4 weeks depending on the response.
Some patients may need higher doses or a shorter interval between the injections. Fluanxol Depot 20mg/ml is unsuitable for patients who require a sedative effect. If volumes larger than 2-3 ml of the 20 mg/ml solution are required the more concentrated solution (Fluanxol Depot 100mg/ml) should be preferred.
When changing the medication from oral Fluanxol to maintenance treatment with Fluanxol Depot the following guidelines should be used: x mg p.o. daily corresponds to 4x mg decanoate every 2 weeks; x mg p.o. daily corresponds to 8x mg decanoate every 4 weeks.
Continue to administer Fluanxol for the first week after the initial injection, then gradually reduce the dosage.
Subsequent doses and intervals between injections should be adjusted according to the patient's response.
Elderly patients: Caution must be exercised in elderly patients.
Renal impairment: Can be given in normal doses.
Liver impairment: Caution must be exercised in patients with hepatic impairment. Careful dosing and, if possible, a serum level determination is advisable.
Children: Flupentixol decanoate is not recommended for use in children due to lack of clinical experience.
Method of administration: Flupentixol decanoate is administered by intramuscular injection into the upper outer quadrant of the gluteal region. Injection volumes exceeding 2 ml should be distributed between two injection sites. Local tolerability is good.
Symptoms of an overdose are unlikely due to the method of administration.
Symptoms: Somnolence, coma, extrapyramidal symptoms (movement disorders), convulsions, shock, hyperthermia or hypothermia.
ECG changes, QT prolongation, Torsade de Pointes, cardiac arrest and ventricular arrhythmias have been reported following an overdose of flupentixol by patients who are concurrently taking drugs known to affect the heart.
Treatment: Treatment is symptomatic and supportive. Gastric emptying should be carried out as soon as possible following oral ingestion, and activated charcoal may be given. Steps should be taken to support the respiratory and cardiovascular systems. Epinephrine (adrenaline) must not be used, as it may further lower the blood pressure. Convulsions can be treated with diazepam and extrapyramidal symptoms with biperidine.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Decreased level of consciousness regardless of cause (for instance intoxication with alcohol, barbiturates or opiates), circulatory collapse or coma.
Neuroleptic malignant syndrome characterised by hyperthermia, muscle rigidity, autonomic dysfunction, impaired level of consciousness and increased serum levels of creatine kinase have been reported with antipsychotic agents.
The risk may possibly increase with drug potency.
Patients with pre-existing organic brain syndrome, mental retardation, and opiate or alcohol misuse are overrepresented among the fatal cases.
Treatment: Discontinuation of antipsychotics, symptomatic and general supportive in-patient treatment. The symptoms may persist for over a week following withdrawal of oral antipsychotics and somewhat longer with prolonged release formulations.
Caution must be exercised when using Flupentixol in patients with organic brain syndrome, convulsions and advanced liver disease.
Flupentixol in doses up to 25 mg daily is not recommended in excited or overactive patients, since the activating effect of the product can exacerbate these symptoms. When the patient is already being treated with sedatives or neuroleptic agents with a sedative effect, these should be gradually withdrawn.
Insulin and glucose response may be altered, and patients with diabetes may require adjustment of their hypoglycaemic treatment.
To determine whether the maintenance dose can be reduced, patients receiving long-term therapy, especially in high doses, should be monitored carefully at regular intervals.
Flupentixol may cause QT prolongation. Persistently prolonged QT intervals may increase the risk of malignant arrhythmias. Flupentixol should therefore be used with caution in susceptible individuals (patients with hypokalaemia, hypomagnesaemia or a genetic predisposition to arrhythmia) and in patients with a history of cardiovascular disorders such as QT prolongation, excessive bradycardia (< 50 beats per minute), a recent acute myocardial infarction, untreated heart failure or cardiac arrhythmia.
Concomitant treatment with other antipsychotics should be avoided (see Interactions).
Cases of venous thromboembolism (VTE) have been reported with antipsychotic drugs. Since patients treated with antipsychotics often present with acquired risk factors for VTE, all possible risk factors for VTE should be identified before and during treatment with flupentixol and preventive measures undertaken.
Leukopenia, neutropenia and agranulocytosis have been reported with antipsychotics, including zuclopenthixol decanoate.
Long-acting depot antipsychotics should be used with caution in combination with other medicines known to have a myelosuppressive potential, as these cannot rapidly be removed from the body in conditions where this may be required.
Effects on ability to drive and use machines: Fluanxol Depot may have minor or moderate effect on the ability to drive vehicles and use machines, especially at the start of treatment or at dose increments.
Use in the Elderly: Cerebrovascular: Flupentixol should be used with caution in patients with risk factors for stroke.
An approximate 3-fold increased risk of cerebrovascular adverse events has been seen in randomised placebo-controlled clinical trials in the dementia population with some atypical antipsychotics. The mechanism for this increased risk is not known. An increased risk cannot be excluded for other antipsychotics or other patient populations.
Increased Mortality in Elderly people with Dementia: Data from two large observational studies showed that elderly people with dementia who are treated with antipsychotics are at a small increased risk of death compared with those who are not treated. There are insufficient data to give a firm estimate of the precise magnitude of the risk and the cause of the increased risk is not known.
Flupentixol is not licensed for the treatment of dementia-related behavioural disturbances.
Fertility: In humans, adverse events such as hyperprolactinaemia, galactorrhoea, amenorrhoea, erectile dysfunction and ejaculation failure have been reported (see Adverse Reactions). These events may have a negative impact on female and/or male sexual function and fertility.
If clinically significant hyperprolactinaemia, galactorrhoea, amenorrhoea or sexual dysfunction occur, a dose reduction (if possible) or discontinuation should be considered. The effects are reversible on discontinuation.
In preclinical fertility studies in rats, flupentixol slightly affected the pregnancy rate of female rats. Effects were seen at doses well in excess of those applied during clinical use.
Pregnancy: Fluanxol Depot should not be used during pregnancy unless clearly necessary.
Neonates exposed to antipsychotics (including Fluanxol Depot) during the third trimester of pregnancy are at risk of adverse reactions including extrapyramidal and/or withdrawal symptoms that may vary in severity and duration following delivery. There have been reports of agitation, hypertonia, hypotonia, tremors, somnolence, respiratory distress, or feeding disorder. Consequently, newborns should be monitored carefully.
Animal studies have shown reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Lactation: Fluanxol Depot should only be used during lactation when clinical assessment reveals a compelling indication, but it is advisable to monitor the child, especially in the first 4 weeks after birth.
Concentrations of Fluanxol Depot detected in breast-milk are so low that they are unlikely to affect the child at therapeutic doses.
The dose that the child ingests is less than 0.5 % of the weight-related daily dose taken by the mother (see Pharmacology: Pharmacokinetics under Actions).
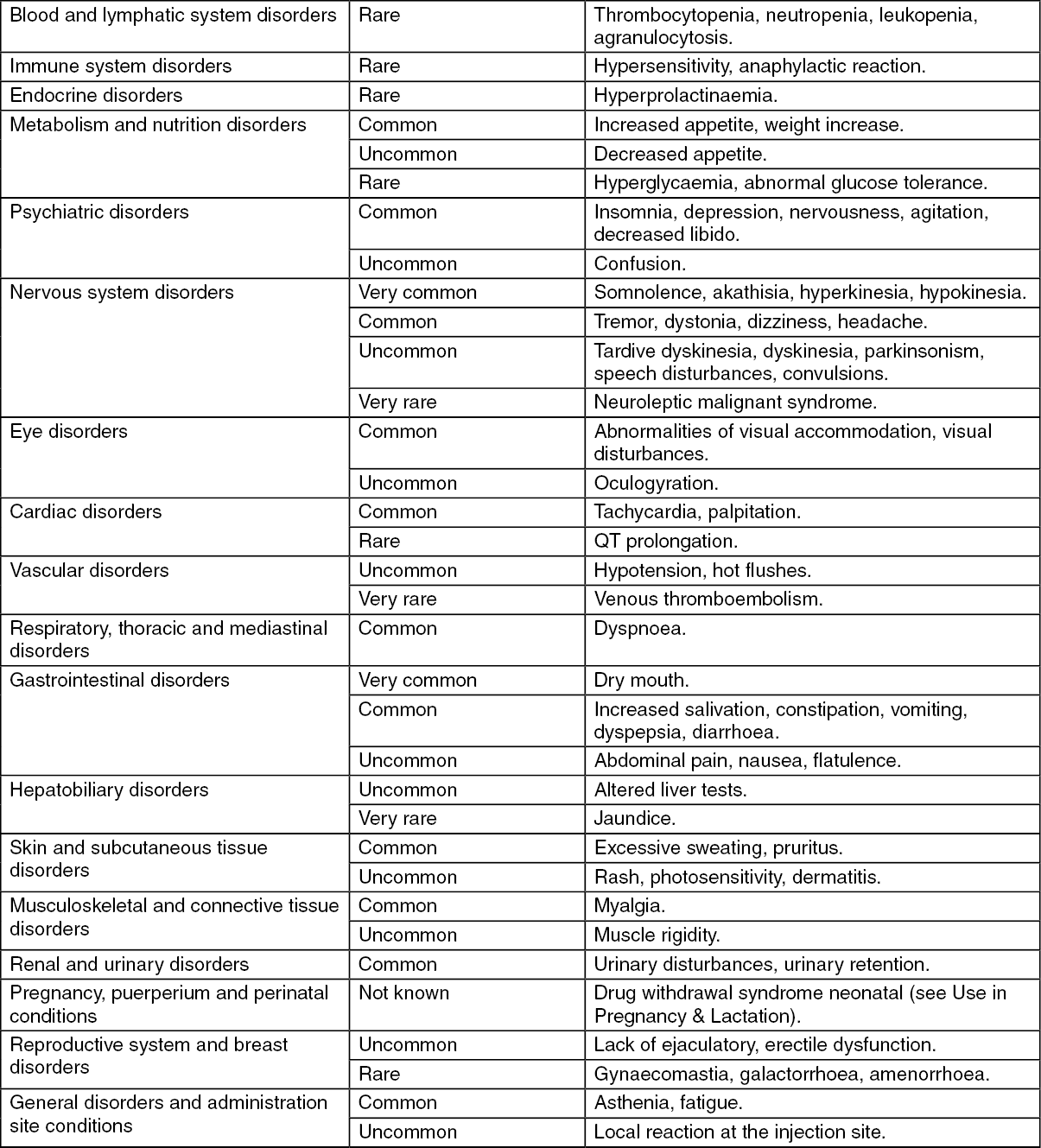
The most common side effects are dry mouth, somnolence, akathisia, hyperkinesia and hypokinesia, which are likely to occur in fewer than 10 % of the patients treated.
Undesirable effects are for the most part dose-dependent. They are more frequent and more severe at the start of treatment and will usually diminish with continued treatment.
Movement disorders may occur, especially at the start of treatment. In the majority of cases these adverse reactions can be satisfactorily remedied by reducing the dose and/or using of antiparkinson agents. Routine prophylactic use of antiparkinson agents is not recommended. Antiparkinson agents do not relieve tardive dyskinesias, but can worsen the symptoms. Dose reduction or, if possible, discontinuation of therapy is recommended. A benzodiazepine or propranolol may be beneficial in patients with persistent akathisia.
Frequencies are taken from the literature and spontaneous reporting. Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), or not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
As with other antipsychotics, rare cases of QT prolongation, ventricular arrhythmias such as ventricular fibrillation and ventricular tachycardia, Torsade de Pointes and sudden unexplained death have been seen in connection with flupentixol (see Precautions).
Sudden discontinuation of flupentixol may give rise to withdrawal symptoms. The most common symptoms are nausea, vomiting, anorexia, diarrhoea, rhinorrhoea, sweating, myalgias, paraesthesias, insomnia, restlessness, anxiety and agitation. Patients may also experience vertigo, may feel warm/cold, respectively, and experience tremor. The symptoms usually set in 1-4 days after discontinuation and subside during 1-2 weeks.
Flupentixol may potentiate the sedative effect of alcohol and the effects of barbiturates and other CNS depressants. Antipsychotic agents may increase or reduce the effect of antihypertensive agents. They reduce the antihypertensive effect of guanethidine and similar agents.
Concomitant use of antipsychotics and lithium increases the risk of neurotoxicity. The metabolism of tricyclic antidepressants is inhibited by antipsychotics and vice versa.
Flupentixol may reduce the effect of levodopa and adrenergic agents.
Concomitant use of metoclopramide and piperazine increases the risk of extrapyramidal problems.
Co-administration of medicinal products known to prolong the QT interval is not recommended (see Precautions). Relevant classes include: class Ia and III antiarrhythmics (e.g. quinidine, amiodarone, sotalol); certain antipsychotics (e.g. thioridazine); certain macrolides (e.g. erythromycin); certain antihistamines (e.g. terfenadine, astemizole); certain quinolone antibiotics (e.g. moxifloxacin).
The previously mentioned list is not exhaustive, and other medicinal products known to cause significant QT prolongation (e.g. cisapride and lithium) should be avoided.
Agents known to cause electrolyte disturbances such as thiazide diuretics (for hypokalemia) and agents known to increase the plasma levels of flupentixol should also be used with caution concurrently with flupentixol, as they may increase the risk of QT prolongation and malignant arrhythmias (see Precautions).
Special precautions for disposal: Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Do not be mixed with other solution for injection.
Do not store above 25°C.
Keep the ampoules in the outer carton in order to protect from light.
Shelf life: 4 years.
N05AF01 - flupentixol ; Belongs to the class of thioxanthene derivatives antipsychotics.
Fluanxol Depot inj 20 mg/mL
1 mL x 10 × 1's;2 mL x 10 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
